Troponin assays have been the biomarker of choice for Acute Coronary Syndrome (ACS) risk stratification for the past two decades and have always been viewed as a bit of the objective metric within ACS pathways. They are very specific for myocardial injury, but not for the cause. The initial (conventional) assays really lacked the sensitivity for a rule out in a timely fashion. In 2007, high sensitivity troponin assays were first released on the market. These assays are highly precise at very low levels of troponin in serum. And by definition, they’re able to detect troponin in 50% of a normal population. So they often will require a repeat or a delta troponin if the value comes in above the level of detection. We look for a change to determine whether it is an acute or chronic injury pattern, these are terrific in terms of negative predictive value for non-ST elevation myocardial infarction and also they allow us to identify non-STEMI earlier than previously so we can start treatment earlier. They also though reveal previously hidden myocardial injury, which we are still not really that well advised as to what to do about. Because of this, there has been slow uptake in the use internationally and this is largely because there’s limited clinical evidence to help us with interpreting how to interpret the values.
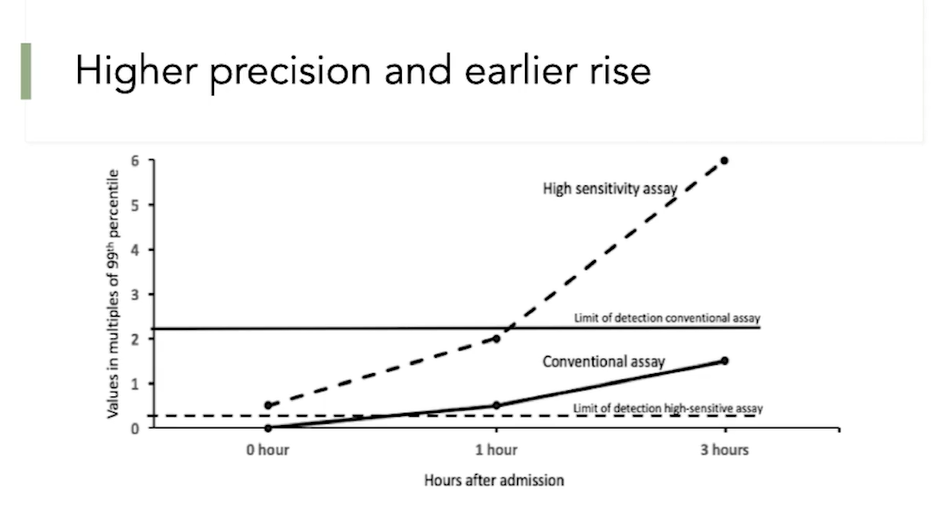
So I’ll just briefly go through the differences between the higher sensitivity troponin and our conventional troponin. As you can see on the Y-axis, that’s the level of troponin, and then, the X-axis is over time. The solid black line is the limit of detection of the conventional assay. The solid curve here represents the clinical assay and as you can see, it’s starting to rise at about three hours, but it does not cross its limit of detection until well after three hours, generally six, but doesn’t reach true sensitivity for twelve hours. In contrast, the high sensitivity assay which is represented by the dotted line here, has a limit of detection, which is all the way down here. And as you can see, it very rapidly crosses the limit of detection and it starts to rise and can give us information about myocardial injury in the patient.
In South Australia, we had been using the conventional fourth generation troponin assay. In 2011, this was replaced with the high sensitivity, or the fifth generation assay. There were a lot of concerns about how we were going to interpret these results and the biggest concern was that we’re going to overwhelm the system with patients for further investigation. So the decision was made by the health department, to mask the high sensitivity results from the clinicians and would continue to report the values in a conventional format despite using a high sensitivity assay. Prior to 2011, we had the conventional assay which reported down to 29 nanograms per litre, we had no information below that.
In 2011 all our assays throughout South Australia were replaced with a high sensitivity assay, which we’re giving us results all the way down to the limit of blank which is 3, but reporting to less than the limit of detection which is 5. Due to the concerns about how do we interpret this and fear that we were going to suddenly rush the system with many tests needed to be done after ED presentation, the values below 29 nanograms per litre on the high sensitivity assay were not reported to clinicians, they were blinded. So, everything was just reported as less than 29 nanograms per litre.